
{kind=link}
The idea that all people have an innate “gender identity” recently has been endorsed by many health-care professionals and mainstream medical organizations. This term commonly is defined to mean the “internal, deeply held” sense of whether one is a man or a woman (or, in the case of children, a boy or a girl), both, or neither. It also has become common to claim that this sense of identity may be reliably articulated by children as young as three years old.
While these claims about gender identity did not attract systematic scrutiny at first, they now have become the subject of criticism from a growing number of scientists, philosophers and health workers. Developmental studies show that young children have only a superficial understanding of sex and gender (at best). For instance, up until age seven, many children often believe that if a boy puts on a dress, he becomes a girl. This gives us reason to doubt whether a coherent concept of gender identity exists at all in young children. To such extent as any such identity may exist, the concept relies on stereotypes that encourage the conflation of gender with sex.
However, starting at a young age, children do tend to exhibit preferences and behaviors that we associate with sex (as distinct from gender). For example, male children display more aggressive behavior than female children. In addition, “cross-sex” behavior—or, more accurately, cross-sex stereotypical behavior—often is predictive of later same-sex attraction.
Can all of these findings be integrated? To start, just as sex influences the development of bodies, it also influences brains. There are in-utero differences in hormone exposures (male testosterone surges at eight weeks gestation, for example), and distinct developmental pathways are triggered based on the XX (typically female) or XY (typically male) chromosomal make-up of neurons. The integration of these sex-related and other developmental processes with environmental pressures gives rise to an individual’s unique personality and preferences.
It comes as no surprise then that population-based studies have demonstrated sex-related differences in personality and preferences that are independent of social influences. When social influences are weakened (in more egalitarian societies such as the Nordic countries of Europe), the sex-related differences in personality and preferences actually increase (the opposite of what one would expect if men and women were wired in an identical fashion). This suggests that as environmental pressures become relaxed, innate sex-specific preferences surface.
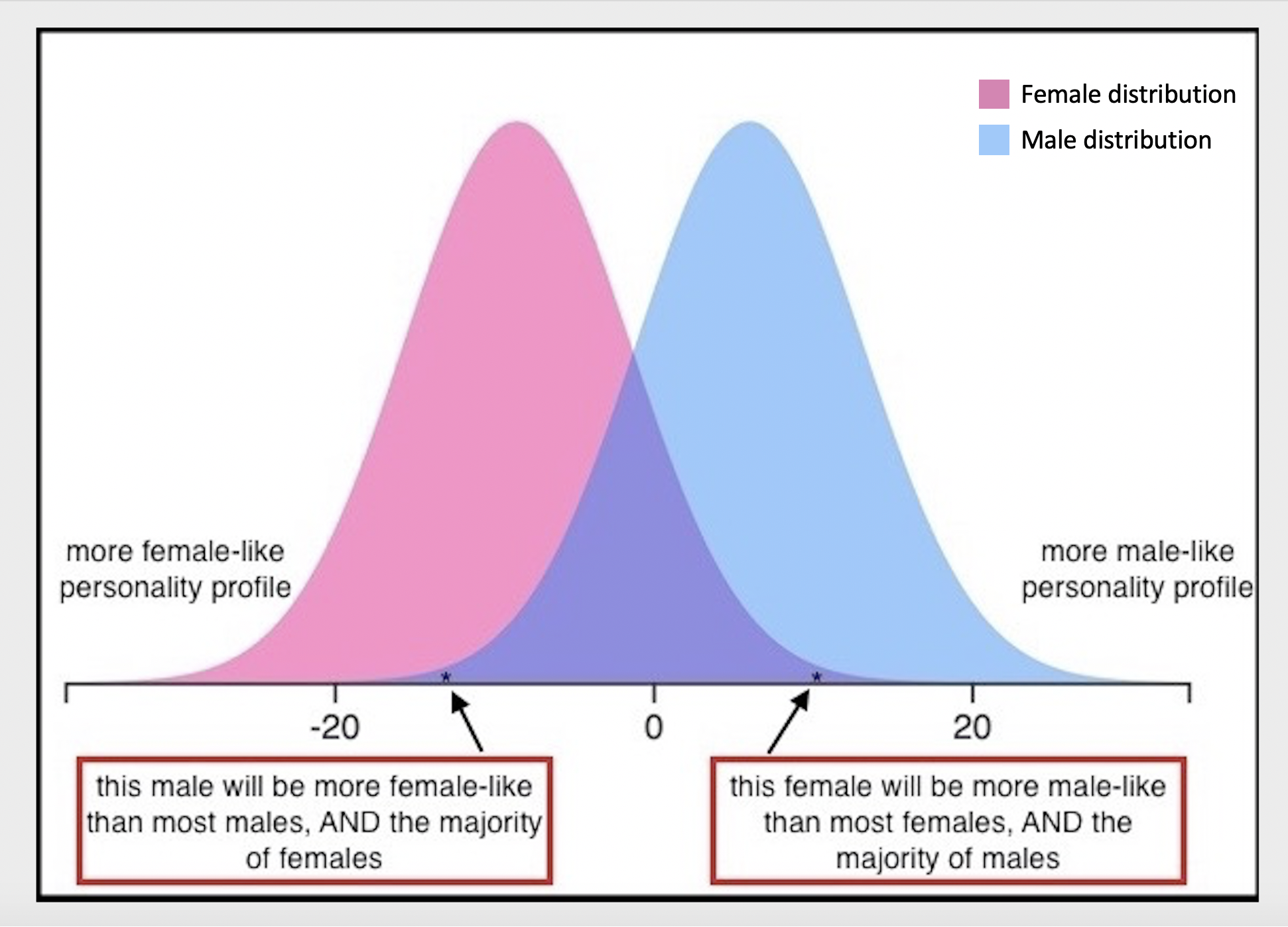
A closer look at personality traits shows that when data is analyzed in aggregate, there is a roughly 30% overlap between sexes, as schematized in the accompanying figure. The consequence of this overlap is that adolescent males who fall on the left end of the male (blue “masculine”) curve, and adolescent females who fall on the right end of the female (pink “feminine”) curve, will exhibit personality traits that diverge from the majority of other members of their own sex. In fact, due to the overlap of personality traits between males and females, the personality traits of some females will be more “male-like” than those exhibited by some, or even most males’ and vice versa.
In the case of an adolescent female whose behavior, personality traits and preferences are more “masculine” than most girls and most boys, she could be led to incorrectly conclude that she is really a male, born in the wrong body. That child’s parents could become confused as well, noticing how “different” their child’s behavior is from their own, or from that of their peers. In reality, that child simply exists at the end of a behavioral spectrum, and “sex-atypical” behavior is part of the natural variation exhibited both within and between the sexes. Personality and behavior do not define one’s sex.
There are approximately 40-million children in the United States between the ages of four and fourteen. The distribution curve above would suggest that roughly four-million of them have personality profiles that are “sex atypical,” but which are still part of the natural distribution of personalities within each sex.
The broad, but normal distribution of personality traits also explains studies showing a 28% concordance of transgender identity in twins. Twins have identical chromosomes, and so likely will have similar sex-related behaviors, as well as experience similar environmental influences in regard to those behaviors. Using twin adolescent males as an example: If their behaviors are at the “feminine” end of the male-typical distribution, they could both become confused as to what their behaviors and preferences mean about their sex.
 Quillette
Quillette
In most cases, the thing that is now called “gender identity” likely is simply an individual’s perception of how their own sex-related and environmentally influenced personality compares to same and opposite sexed people. Put another way, it’s a self-assessment of one’s stereotypical degree of “masculinity” or “femininity,” and it’s wrongly being conflated with biological sex. This conflation stems from a cultural failure to understand the broad distribution of personalities and preferences within sexes and the overlap between sexes.
When a girl reports that she “feels like a boy” or “is a boy,” that sentiment may reflect her perception of how her personality and preferences compare to the rest of her peers. If the girl has an autism spectrum condition, she may even perceive “sex-atypical” behavior that does not actually exist, and thereby falsely self-diagnose as male even without experiencing any actual male personality traits.
It should be noted that these scenarios don’t apply to all cases of gender dysphoria, as many other triggers are described in the literature. But in most cases, counseling can help gender dysphoric adolescents resolve any trauma or thought processes that have caused them to desire an opposite sexed body.
Historical data suggests that about 0.5% of children develop gender dysphoria—distress caused by a perceived incongruence between one’s biological sex and gender presentation. Reinforcing studies in the medical literature show that, as children get older, childhood-onset gender dysphoria resolves (i.e. ends) in most cases. As two authors put it in a 2016 International Review of Psychiatry article, “the conclusion from these studies is that childhood GD [gender dysphoria] is strongly associated with a lesbian, gay or bisexual outcome and that for the majority of the children (85.2%; 270 out of 317 [studied individuals]) the gender dysphoric feelings remitted around or after puberty.”
Yet instead of offering counseling, medical professionals now are commonly telling children that they may have been “born in the wrong body.” This new approach, called “gender affirmation,” makes gender dysphoria less likely to resolve, pushing children down the path toward irreversible medical and surgical interventions. If aggressive transition options are pursued early in puberty, the combination of puberty-blocking drugs, followed by cross sex hormones, will result in permanent infertility.
The growing population of transgender-identifying high school students now is estimated to comprise about 2% of all students—a three-fold increase over the baseline 0.5% figure cited above. Many adolescents now are presenting to gender clinics, with some clinics seeing a 10-fold increase in new cases. Many of these adolescents have no history of childhood gender dysphoria. Higher rates of autism-spectrum conditions have been described in many of these adolescents, and the controversial “affirmation model” is being applied to this unstudied cohort as well. Not surprisingly, reports of transition regret, and de-transition, are growing in number.
To summarize, a lack of understanding regarding the distribution of sex-related personality and behavioral differences has led to confusion that impacts children who fall at the extreme tail-ends of the distribution, and who would be statistically more likely to grow up to be gay, lesbian or bisexual adults if allowed to experience uninterrupted puberty. Additionally, telling a child that he or she was born in the wrong body pathologizes “gender non-conforming” behavior and makes gender dysphoria less likely to resolve.
The fact is, no child is actually born in the wrong body. Adults should expand their understanding of what normal male and female behavior and preferences look like—which would lead them to appreciate that being male or female comes with a wider range of personalities preferences, and possibilities than old stereotypes would have us believe.
Keep reading
Antifragility in Ukraine


Richard Dawkins and the Claude Delusion
Open Hiding
The Case Against State-Sanctioned Euthanasia
Lists, Damn Lists, and Critical Correctness
