COVID-19 Updates
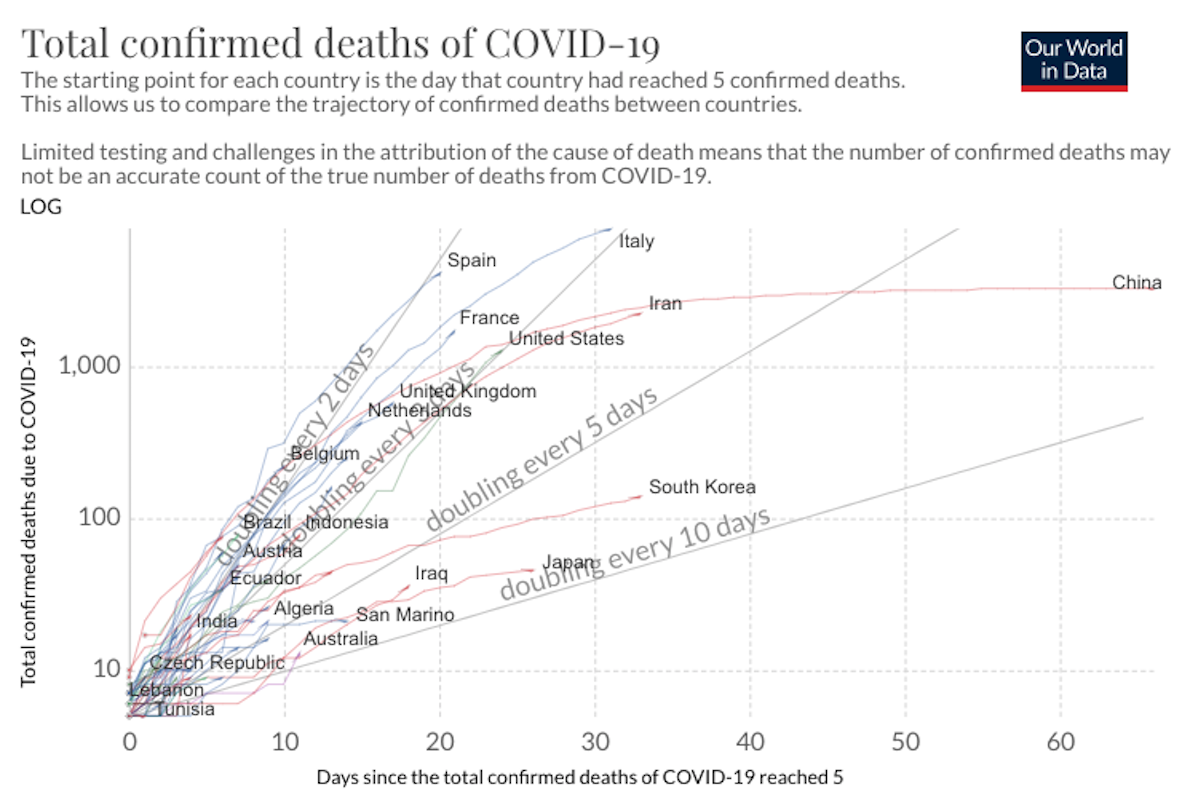
COVID-19 Science Update for March 27th: Super-Spreaders and the Need for New Prediction Models
Absent isolation or other precautionary measures, the average socially active COVID-19 infectee will transmit the disease to an average of about 2.4 people. i.e., the R0 value is 2.4. But super-spreaders can spread a disease to dozens or hundreds.
· 11 min read
{kind=link}
Keep reading
Criminal Research
Rosalind Arden
· 14 min read

Getting Away With It
Andrew Bushnell
· 11 min read

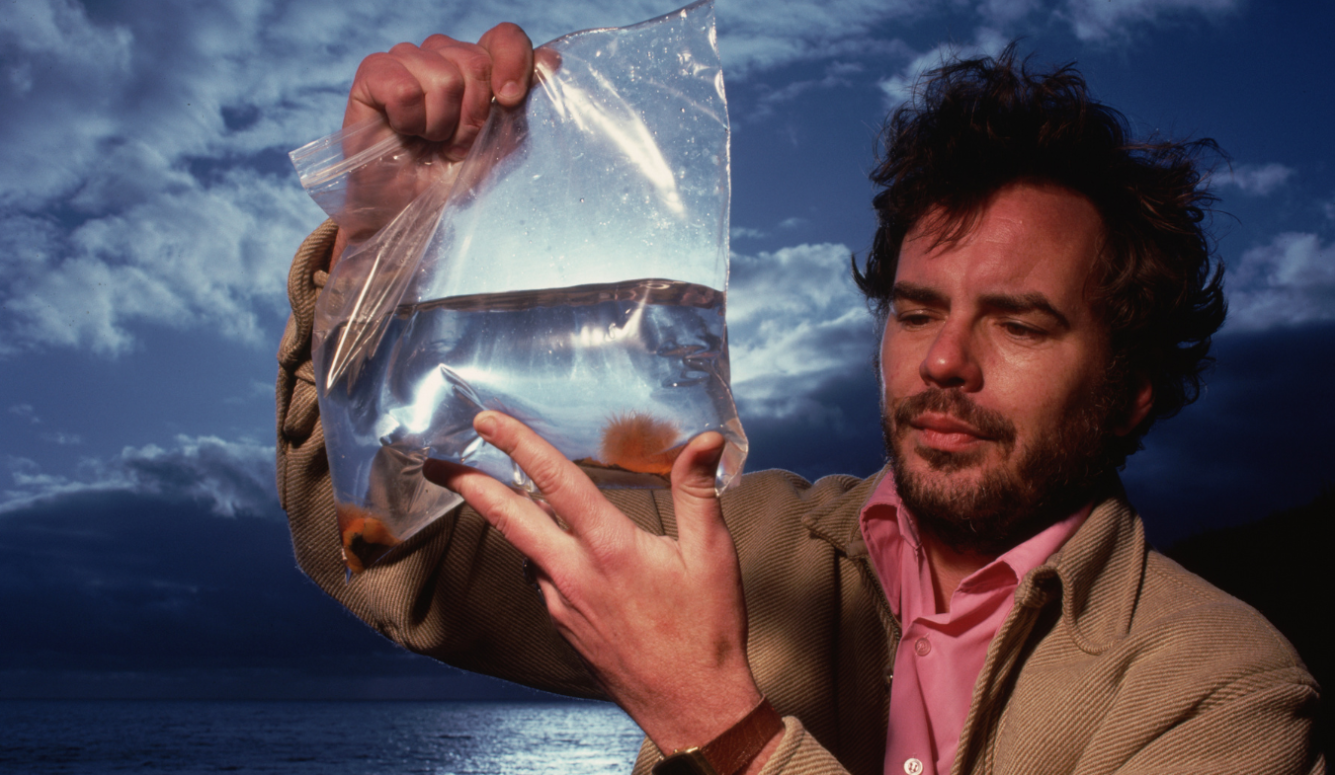
The Many Roots of Our Suffering: Reflections on Robert Trivers (1943–2026)
Steven Pinker
· 16 min read
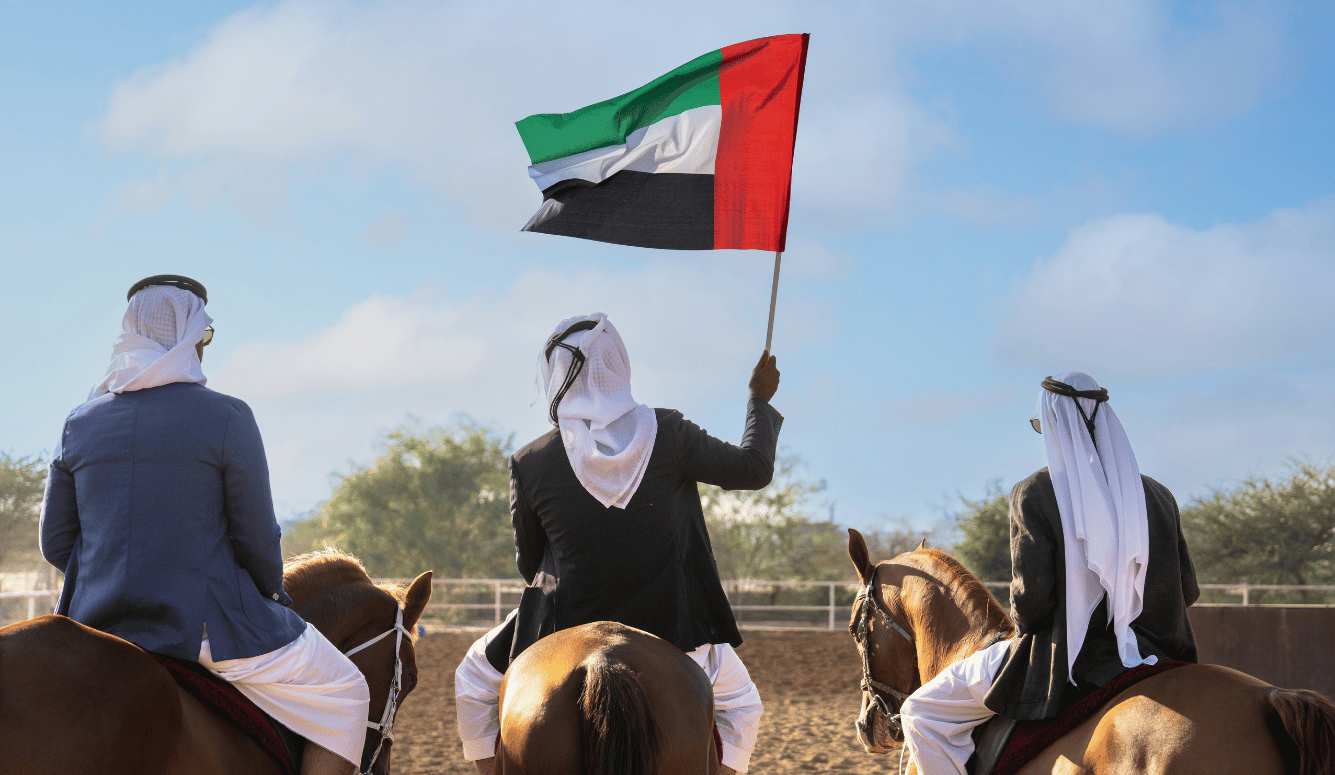
The First Post-Ideological Bedouin State
Chama Mechtaly
· 12 min read
Trump, Tehran, and the China Calculus
Aaron Sarin
· 7 min read
