Transgender
The Cass Effect
A landmark report properly emphasises the application of science, not slogans, in establishing treatment protocols for trans-identified children.

{kind=link}
On 10 April, Dr Hilary Cass, a former president of Britain’s Royal College of Paediatrics and Child Health, released the Final Report following her Independent Review of Gender Identity Services for Children and Young People. While Dr Cass’s formal mandate was limited to providing recommendations regarding the treatment of gender dysphoric children by England’s National Health Service, her report’s publication has rightly been treated as important international news.
The need for an authoritative and objective assessment of medical practices in this area has been obvious for years, notwithstanding oft-repeated reassurances that therapists and doctors have no higher duty than to simply “affirm” the asserted identities of trans-identified children. Doing otherwise, we’ve been instructed by professional organisations such as the World Professional Association for Transgender Health (WPATH), would endanger the emotional health of gender dysphoric children, and possibly even drive them to suicide. But, as Dr Cass shows, this morbid rhetoric doesn’t accurately reflect the available evidence. And her analysis should serve to inform policy-reform efforts all over the world.
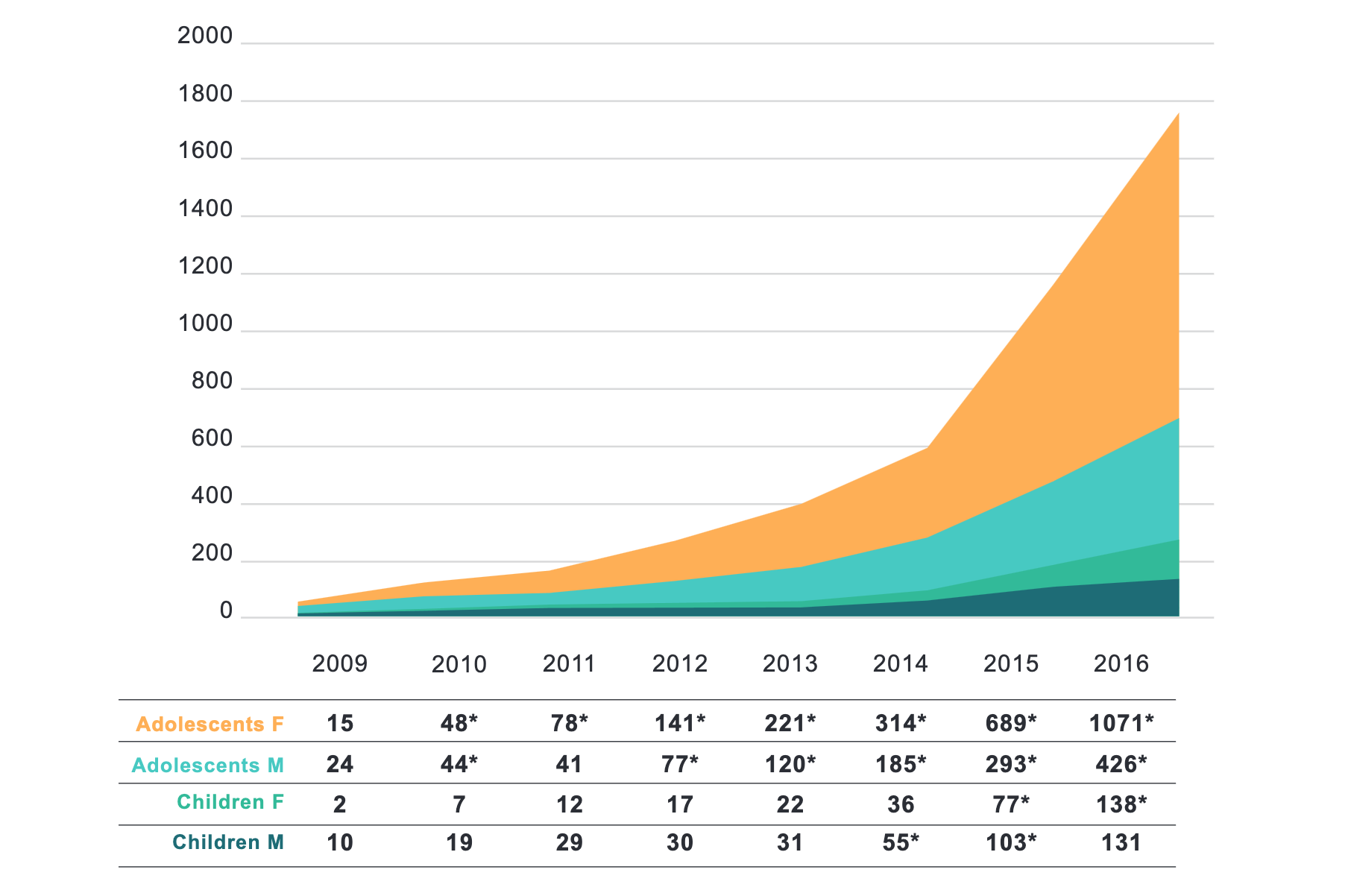
As Dr Cass reports, the number of children claiming to experience gender dysphoria began skyrocketing during the 2010s, on a timetable roughly in line with the rise of social media—a phenomenon she contextualises alongside the “substantial increase in rates of mental health problems in children” more generally, especially teenage girls. Echoing the pioneering work of Dr Lisa Littman, Dr Cass notes the effects of “peer influence” and “the rise in young people presenting with other bodily manifestations of distress; for example, eating disorders, tics, and body dysmorphic disorder.”
An important theme running through Dr Cass’s report is that clinicians must assess trans-identified children holistically, through a process that includes a full mental-health assessment. This proposition may seem so obvious as to not require articulation—especially given the high level of psychiatric comorbidity exhibited among trans-identified children (a topic discussed in more detail below). And yet, pro-transition activists typically either ignore this troubling pattern of comorbidity altogether, or seek to cast it as an artefact of transphobia—a strategy of deflection that Dr Cass properly rejects.
 Joseph Elkadi
Joseph Elkadi
In many progressive circles, the rising tide of detransition—by which formerly trans-identified individuals come to accept their biological identity—remains a taboo topic, as it undercuts the fashionable conceit that each child possesses an unerring (and therefore unfalsifiable) sense of his or her own authentic “gender identity.” Dr Cass dispenses with this taboo, as well. Notably, the word “detransition” appears over 300 times in her report.
Most importantly, Dr Cass rejects the dangerous myth that puberty blockers are known to be harmless drugs that merely hit the “pause” button on biological development. On this score, the summary points numbered 81 through 83 in her report are instructive:
[A] systematic review… found multiple studies demonstrating that puberty blockers exert their intended effect in suppressing puberty, and also that bone density is compromised during puberty suppression. However, no changes in gender dysphoria or body satisfaction were demonstrated. There was insufficient/inconsistent evidence about the effects of puberty suppression on psychological or psychosocial wellbeing, cognitive development, cardio-metabolic risk, or fertility. Moreover, given that the vast majority of young people started on puberty blockers proceed from puberty blockers to masculinising/feminising hormones, there is no evidence that puberty blockers buy time to think, and some concern that they may change the trajectory of psychosexual and gender identity development.
Overall, Dr Cass found that the “potential risks to neurocognitive development, psychosexual development, and longer-term bone health” associated with puberty blockers are substantial, and require further investigation. Moreover, while “it has been suggested that hormone treatment reduces the elevated risk of death by suicide in this population,” the available evidence “did not support this conclusion.”
Dr Cass’s bottom-line recommendation is that England’s National Health Service (NHS) adopt “an extremely cautious” approach, by which “a strong clinical rationale” is required before providing hormones to anyone younger than eighteen years of age—a recommendation that the NHS has already indicated it will be implementing. Going forward, the only trans-identified minors to receive puberty blockers through the NHS will be those participating in clinical trials. And Holyrood has followed suit—a striking development given Scotland’s unusually fervent embrace of trans-activist demands in the past.
Keep reading
Treating Myths as Science

The Edifice Complex
Letters to the Editor
Criminal Research

Getting Away With It