Bioethics
Looking for COVID-19 ‘Miracle Drugs’? We Already Have Them. They’re Called Vaccines
The evidence that mRNA-based COVID-19 vaccines are safe, and that they work, is about as solid as medical evidence gets.
{kind=link}
Bret Weinstein, a former professor of biology at Evergreen State College, is best known for being hounded off his own campus in 2017 by a horde of social-justice zombies who themselves seemed to resemble nothing so much as a lab accident gone wrong. Having become a martyr of hyper-progressive ideological mania, Weinstein resigned, sued, won, starred in a documentary about the experience, and embarked upon a new career as a podcaster.
Since then, Weinstein has become both a symbol and a voice for millions of Americans, on the Left and Right alike, who are unnerved that a handful of Silicon Valley oligopolists have acquired the power to set the boundaries of acceptable speech, if not formally, then effectively. Weinstein has become an influential public figure, with 350,000 subscribers on YouTube. Many consider his voice a credible one in life-and-death debates about the COVID-19 pandemic.
Recently, Weinstein has graduated from entertaining theories that might not be right but could do no harm, to theories that cannot be right and are sure to do harm. Because of Weinstein’s prominence, and the trust his listeners place in him, this harm can be measured and is considerable. His promotion of outright quackery, during a pandemic that has killed more Americans than any catastrophe since the Civil War, is immoral.
In early June, Weinstein began to claim that ivermectin—a genuinely remarkable antiparasitic drug used to treat tropical diseases such as river blindness—could be applied to “eradicate” COVID-19. He invited physicians from a group called the Front Line COVID-19 Critical Care Alliance (FLCCC) to join him in what he called “an emergency podcast” to “save the world.” He began by explaining gravely that “something very serious is afoot, and the public is largely unaware that they have been placed into a kind of danger.” He and his guests offered the claim that ivermectin is “99 percent effective” in treating COVID-19; that it could be used as a prophylaxis against infection; and that were it widely used, the pandemic would end in “a month.” These truths, they suggested, had been suppressed by a conspiracy. They did not specify the mechanism by which the supposed conspiracy works, but they were clear about its object: selling COVID-19 vaccines.

YouTube, rotely enforcing its Terms of Service provisions and COVID-19 medical misinformation policy (these are very explicit and detailed) promptly took the podcast down. To Weinstein and many of his followers, this was evidence of the conspiracy.
Had Weinstein stopped there, it would have been nutty, destructive, and misleading, but otherwise inoffensive. Ivermectin is generally a safe drug. It’s unlikely his listeners will kill themselves with it. It’s the next step he took that’s so deadly: On the same podcast, he and his guests argued that the Pfizer and Moderna mRNA vaccines authorized for use in the United States, as well as the AstraZeneca adenovirus-vector vaccine, are so unsafe that the vaccinated are secretly dropping like flies from their effects. He also has avowed, on both the podcast and his Twitter feed, his trust in a UK physician named Tess Lawrie who has published a phenomenally insane paper that calls COVID-19 vaccines “unsafe for human use.” The paper advises that “Preparation should now be made to scale up humanitarian efforts to assist those harmed by the COVID-19 vaccines.”
Weinstein and another physician affiliated with the FLCCC, American critical-care physician Pierre Kory, then visited Joe Rogan’s podcast to argue that because large pharmaceutical companies make more money by bringing new, untested drugs to the market than by selling repurposed drugs such as ivermectin, they have convinced government officials and social-media companies to obscure or suppress the evidence of the trail of death and misery these COVID-19 vaccines are leaving in their wake.

It is Weinstein’s right under the First Amendment to say all of this. But let’s not confuse a right to say something with something being right to say. The consequences of Weinstein’s caper will be ruinous. COVID-19’s Delta variant, twice as contagious and possibly more lethal than the original strain, is ravaging the world. Its effects have been devastating in India, and among the unvaccinated in the UK.
Indian hospitals have reported a high case load of pediatric mortality and morbidity. That children can die from COVID-19 is a point worth stressing, given the emphasis that Weinstein and other vaccine skeptics have placed on the vaccines’ risks to children. The impression listeners might get from Weinstein’s podcast is that children are at no risk from this disease. This is false. A retrospective cohort study published recently in Nature found that among 12,306 lab-confirmed pediatric COVID-19 patients in the United States, in the study cohort, the hospitalisation frequency was 5.3 percent, with 17.6 percent needing critical care services and 4.1 percent requiring mechanical ventilation. We don’t know how many cases go unconfirmed, so this study leaves important questions unanswered. But clearly, COVID-19 is a killer: Last year, it made the top-10 list of causes of pediatric death in the United States. If even a few thousand of Weinstein’s listeners have been convinced by him to avoid being vaccinated, we can reasonably estimate, based on the patterns of infection we’ve so far seen, that many of them will acquire the disease, and roughly 1.8 percent of those will die. Not some, but many of the survivors will suffer permanent damage.
There are risks associated with COVID-19 vaccines, of course. They are well-documented. Most significantly, rare blood-clotting disorders have been tentatively linked to the AstraZeneca (AZ) vaccine. We write “tentatively” because the numbers are so small that it is hard to know if the link is statistically meaningful. As of March 16th, some two million people in Europe and neighboring countries had received the AZ vaccine; of these, five people (yes, just five) below the age of 50 developed disseminated intravascular coagulation—blood clots in multiple blood vessels—within 14 days. Compared to pre-COVID figures, this is five times the epidemiological baseline. But these numbers are so small—five cases observed, versus one expected—that we can’t be confident of a causal relationship. (Epidemiologists have long understood that disease clusters can occur by chance.)
Here is the key point: COVID-19 itself causes blood clots. Study upon study has confirmed this. A meta-analysis published in November concluded that one in five COVID-19 patients develop blood clots. This risk is orders of magnitude greater than any blood-clot risk associated with vaccination. If there were no pandemic, Weinstein and other vaccine skeptics would be perfectly right to say that getting vaccinated is riskier than not getting vaccinated. But why would one be vaccinated at all if there had been no pandemic to begin with? We don’t live in a fictional universe: There is a pandemic, and a deadly one.
The only pandemic-afflicted world to which Weinstein’s eccentric risk analysis would apply is one in which some other, safer drug or therapy prevented or cured COVID-19 without vaccines. So back to ivermectin, which has shown promise in some studies and flopped in others. The quality of the evidence for its efficacy is limited and low. Some studies that sounded promising collapse on closer inspection. On Weinstein’s podcast, for example, listeners were told of an “Argentinian” study, presumably a reference to a November 20 paper entitled Study of the Efficacy and Safety of Topical ivermectin + Iota-Carrageenan in the Prophylaxis against COVID-19 in Health Personnel (often referred to as the IVERCAR study). Lead author Héctor Carvallo, an Internal Medicine specialist, and three other authors report recruiting 1,195 health-care workers from four major Argentinian hospitals, of whom 788 were given a combination drug regimen that included ivermectin. They say that after three months, the 407 workers who did not receive ivermectin had an infection rate of about 58 percent. Among the 788 workers who received ivermectin, the infection rate, they reported, was zero—no cases observed whatsoever.
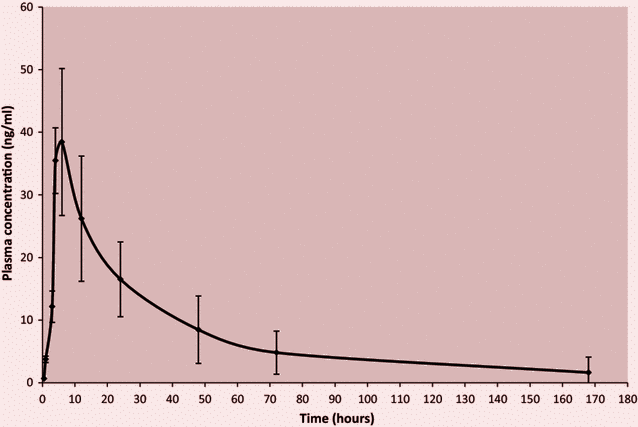
Does this pass the smell test? Not at all. In the initial phase of the study, the workers who received ivermectin were dosed every four hours for two weeks. We’re asked to believe that none of these workers tested positive for SARS-CoV-2 (the virus that causes COVID-19) during this two-week period. We’re also asked to accept that none tested positive during the three weeks that followed. What’s the problem with this? The measured half-life of ivermectin is only about 18 hours. In a follow-up study, the authors replaced the five-times-a-day regimen with a once-weekly dose. Apparently, the control group in one of the hospitals reported a 92 percent incidence of new infections while the ivermectin group again reported zero. If this were true, ivermectin would indeed be a miracle drug—in the very narrow sense of the word, because there’s no physical way it could work like this.
A systematic review of all available research, published in the BMJ, concluded that it was “very uncertain whether ivermectin … reduces the risk of laboratory confirmed infection,” in part “because of serious risk of bias and very serious imprecision” in the studies so far conducted. Does this mean it doesn’t work? No. It means we do not know. This might explain why the FDA “has not approved ivermectin for use in treating or preventing COVID-19 in humans.” The thesis is much more plausible than the notion of a massive conspiracy involving a vast number of people and institutions, all behaving in ways contrary to the interests of humanity, to pad the pockets of Big Pharma.
In Canada, similarly, a provincial review of all available studies found no basis for recommending ivermectin outside of a clinical trial. They specifically note the “critically low quality” of Dr. Tess Lawrie’s meta-analysis.
No one is arguing against ivermectin as a means to help fight COVID-19. We wouldn’t be surprised if it proves to be a useful therapeutic, on its own or in some combination of drugs. If it’s even marginally beneficial, tens of thousands of lives might be saved as the world waits, in desperation, for vaccines. Even if it’s not effective at all, the placebo effect could offer real benefits to patients who sincerely believe it’s a miracle drug.
But it isn’t a sugar pill. To achieve the effects ivermectin has been shown to have on the virus in cultured monkey cells in a laboratory, ivermectin must be taken at doses far above the dose we know to be safe. It causes testicular dysfunction, which is why it’s often prescribed with vitamin E and selenium to prevent testicular toxicity (and nota bene: deficiencies of selenium may result in worse outcomes among COVID-19 patients, a confounding variable for which the studies we have do not account). Ivermectin is a known teratogen: It is dangerous for pregnant women to be exposed to it, no less to take it, especially in high doses. Predictable reports of liver failure owing to self-administered ivermectin have already made the news. The drug has been linked to rare but serious neurological adverse events.
The excitement surrounding ivermectin originated in a study published by Australian researcher Leon Caly and co-authors showing that if you take cells derived from the kidney of an African green monkey, infect them with SARS-CoV-2, and dose them with very high concentrations of ivermectin, the virus is reduced, within 48 hours, to insignificance. But the dose levels required to achieve these results through in vitro experiments are vastly higher than the maximum reported plasma concentration we can achieve in human subjects, a level that is itself many times higher than the safe dose for anti-parasitic uses. Killing viruses in vitro is much easier than doing the same thing in vivo without also killing the organism. Often, cell or animal studies in vitro offer promising results but yield no benefit in humans. And adverse effects, or a lack thereof, in animals do not necessarily translate to the same effect in humans.
But let us say, for argument’s sake, that taking ivermectin at the required dosage were safe and practical. And let’s also imagine that it may be effective at preventing and treating COVID-19. Should those of us lucky enough to live in countries with access to mRNA-based vaccines take ivermectin instead? No: That would be bonkers.
 Iosif M. Gershteyn
Iosif M. Gershteyn
The evidence that mRNA-based COVID-19 vaccines are safe, and that they work, is about as solid as medical evidence gets. Sure, no one can prove that in 10 years’ time, you won’t suffer ill effects. But nor is there any reason to fear this.
We don’t know if Weinstein endorses a claim offered by one of his guests, Dr. Steve Kirsch, that COVID-19 vaccines have caused more deaths than have all other vaccines “combined over the last 30 years.” But he certainly didn’t dispute it. It apparently does not trouble him that the original source of the claim is a notorious conspiracy-theory site called Infowars, which is owned by Alex Jones; nor that it is demonstrably false; nor that the claim relies on a misunderstanding of the way data is collected by the US Vaccine Adverse Event Reporting System; nor that vaccine skeptics make this claim about every vaccine.
By early June, 1.7 billion doses of these vaccines had been administered around the world—to humans, we stress, because, as Weinstein and his guests correctly point out, this is the most important kind of data. Many well-conducted, randomized, observer-blinded, placebo-controlled trials have shown the vaccines to be more than 90 percent effective on the original strains of the virus, and nearly 100 percent effective in protecting you from the most serious adverse effect of the disease: death. An mRNA vaccine study published in the New England Journal of Medicine, for instance, found 94.1 percent efficacy at preventing COVID-19. Of the 30,420 volunteers who took part in the study, “severe COVID-19 occurred in 30 participants, with one fatality; all 30 were in the placebo group.” The authors report that “aside from transient local and systemic reactions, no safety concerns were identified.” Numerous other studies report similar findings, all based on randomized, high-volume, peer-reviewed studies. (It is still unclear how well the vaccines protect against infection by the Delta variant, but Israel’s health ministry reports that the Pfizer mRNA vaccine is 93 percent effective in preventing serious illness and hospitalisation.) If you’re looking for a “miracle drug” to protect you from COVID-19, look no further: This is it.
How does the evidence for the prophylactic efficacy of ivermectin stack up against the vaccines? It’s not even close. Remember: We don’t yet know that the drug provides any significant benefit. A high-quality study published in JAMA found that in a randomized clinical trial that included 476 patients with mild COVID-19, “a 5-day course of ivermectin, compared with placebo, did not significantly improve the time to resolution of symptoms.” (If you’d like to read a detailed assessment of the methodological problems with many of the ivermectin studies, Australian epidemiologist Gideon Meyerowitz-Katz offers a good rundown.)
But again, for the sake of argument, let’s go with the most generous interpretation of available experimental results. This site, which purports to offer a (highly dubious) “real-time meta-analysis” of ivermectin studies, claims the drug’s aggregated prophylactic efficacy is 85 percent. Even if this were true, this would mean your odds of developing COVID-19 while taking ivermectin are about 6.67 times lower than those of a counterpart in the control group. If you’ve received an mRNA vaccine, however, your odds are 20 times lower. Even if we accept the statistics offered by ivermectin’s most enthusiastic advocates, those very figures indicate that you would get triple the protection from the vaccine. Moreover, to get the protective benefits of ivermectin, you’d have to take it daily for months, years, or decades. Given what we know about American adherence to medication regimes, we can be pretty sure many would stop taking it. Two doses of an mRNA vaccine, by contrast, will protect you for months, and probably years.
Jesse Pelletier
If the evidence changes, our minds will change with it. It may yet be shown that ivermectin cures COVID-19. It may yet be shown that it cures cancer, for all we know. But as of today, we have no good evidence it does, and a lot of evidence that the Delta variant will cause carnage in unvaccinated populations.
The ivermectin brigade is not apt to be persuaded by this. They will insist that the evidence isn’t there yet because researchers didn’t use the right dose levels, or administered it at the wrong time, or that the studies that prove they’re right have been blocked. Or they’ll fall back on the idea that the pharmaceutical companies are powerful enough to force every medical journal and regulatory agency in the world to stand up, salute, and take dictation. They’ll also claim that vaccines make you miscarry (nope), or harm your fertility (no), and curdle your breast milk (sorry). These theories won’t die. But, alas, the same isn’t true of the people spouting them, and those who get taken in.
To put things simply: We have proof that ivermectin is terrific for river blindness and head lice. But if you’re taking it to prevent COVID-19 because you heard it was “99 percent effective” on a podcast—while forgoing an mRNA vaccine, because you think that’s too dangerous—you’ve been misled, and you’re endangering yourself, your family, your community, and your country.
No one disputes Bret Weinstein’s right to embrace the theory that ivermectin is a miracle drug, or to regale his listeners with vaccine horror stories and conspiracy theories. But the rest of us reserve the right to be appalled by his judgment and ethics.
Correction: An earlier version of this article indicated that, according to the indicated presumptions, one’s odds of developing COVID-19 while taking ivermectin would be 6.75 times lower than those of a counterpart in the control group, while the corresponding ratio for those who received an mRNA vaccine would be 19. In fact, the correct figures are 6.67 and 20 respectively.
An earlier version of this article also stated that among children from a retrospective cohort study “almost 18 percent needed critical-care services, and 4.1 percent required mechanical ventilation.” The article has been amended to reflect that in the study cohort, the hospitalisation frequency was 5.3 percent, with 17.6 percent needing critical care services and 4.1 percent requiring mechanical ventilation. Quillette apologises for the error.
Keep reading
Buckley’s Blind Spots

The Art of Not Quite Listening
Hell in North Germany

Why the Islamic Republic Must Fall

Podcast #292: Social Work Without Stereotypes

Purity, Profit, and Politics
