COVID-19 Science Update for March 21st: What Is Germany Doing Right?
There are reports of ventilator shortages, and the possibility of an Italian-style horror show, with doctors deciding whose parents live and whose parents die, seems real.
{kind=link}
The latest global data for COVID-19—updated with reports received on March 21st, 2020—have been published at Our World in Data. Here are some of the numbers and trends that I believe deserve special attention, as well as a brief report on notable regional developments and media analyses. Beginning today, these updates will be published at Quillette in our section marked COVID-19 UPDATES. Please report needed corrections or suggestions to [email protected].
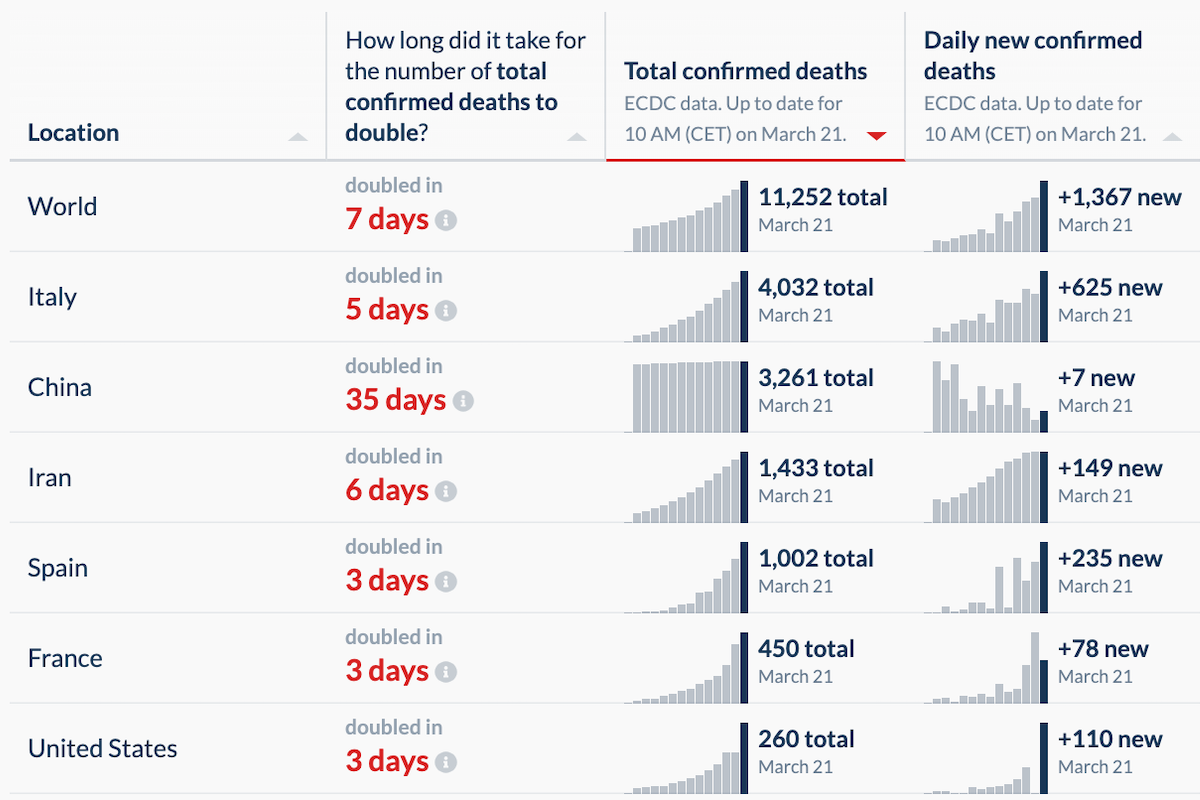
Yesterday’s global tally of confirmed new cases to date was 271,364. This represents a daily jump of 28,891. The previous daily jumps were, proceeding backwards, 29K, 19K, 15K, 12K, and 14K. As has been the case in recent days, the lion’s share of new cases came from just these five countries, which accounted for 74 percent of all new global confirmed cases yesterday:
- France (1.6K new cases, as compared to 1.9K, 1.4K, and 1.1K in the days previous)
- Germany (4.2K new cases, as compared to 5.9K, 1K, and 1.1K in the days previous)
- Italy (6K new cases, following on almost equally massive jumps of 5.3K and 4.2K)
- Spain (2.8K new cases, compared to 3.4K, 2.5K, 2K, 1.4K, 2K, 1.5K, and 1.3K in the week previous)
- United States (5.4K, 4.8K, 3K, and 1.8K in the previous four days).
Obviously, it would be great to see the new-case data flatten and even decline. But the reporting I’ve seen continues to suggest that focusing on new cases can be misleading, since different countries are identifying (and confirming) vastly different proportions of their national caseloads. South Korea, China, and Germany all have tested on a huge scale—a practice that corresponds with relatively high case numbers, but also low observed case-fatality numbers, since thorough testing regimes sweep in mild and asymptomatic cases, and not just the severe and critical ones. (A New York Times report indicates that some of the countries that made an early decision to engage the private sector in testing solutions, such as Australia, South Korea, and Singapore, have been the most agile and effective in testing their citizenry. In New South Wales, Australia alone, 33,000 people have been tested—more than had been tested in all of Canada as of March 15th.)
Keep reading
How Canada Jumped the Rails on ’Gender-Affirming Care’: A Quillette Investigation
In Bad Faith
Letters to the Editor
Dangerous Liaisons and the #MeToo Wars

The Crisis in the Humanities Is Not About Money
