COVID-19
Don't Test, Don't Tell: The Bureaucratic Bungling of COVID-19 Tests
The offenders include rich countries like the United States and Japan, vast countries like Indonesia and India, communist countries like China and Vietnam, theocracies like Iran and Saudi Arabia, oligarchies like Russia and Nigeria, social democracies like Germany and France.

{kind=link}
“I believe that a healthy society should not have only one voice.”
—Li Wenliang, whistleblowing Wuhan physician, killed by coronavirus infection at age 34
On Thursday, February 26th President Donald Trump finished up his initial White House press conference on the coronavirus. He had appointed Vice President Mike Pence as coronavirus czar and spoke about “the fifteen cases that could go to zero.” At the same time, I received a Twitter DM from a physician that included screenshots of an email that had been sent to staff at the UC Davis Medical Center in Sacramento, California earlier that afternoon.
Since that night, the original email has been confirmed by UC Davis and reported on by multiple news organizations. Here’s a copy of the email as reported by NPR.
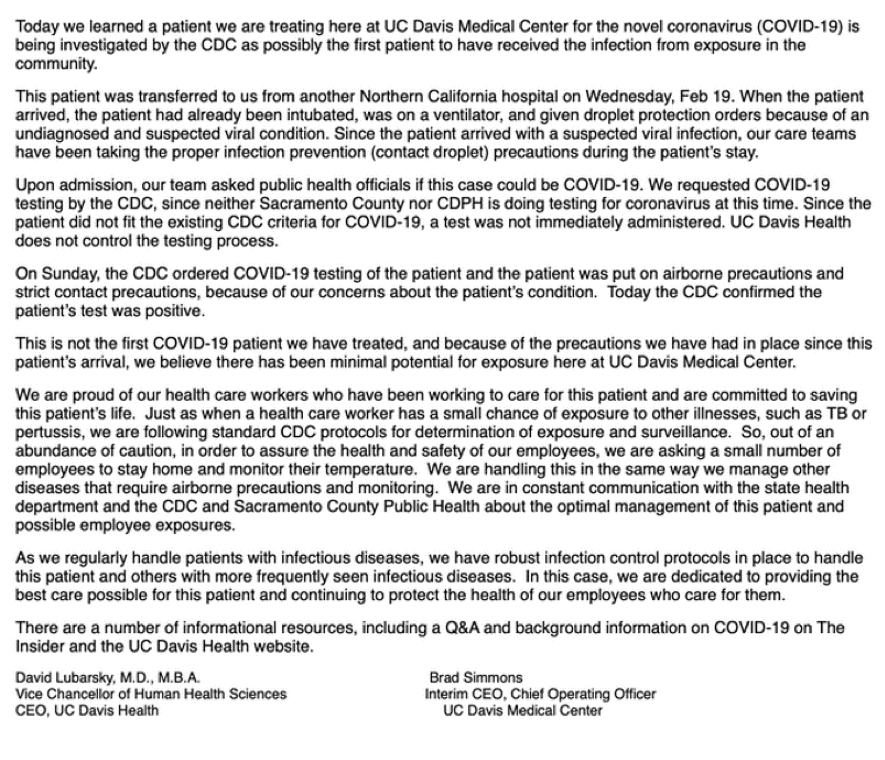
I want to highlight a couple of quotes from this email.
Since the patient did not fit the existing CDC criteria for COVID-19, a test was not immediately administered. UC Davis Health does not control the testing process.
The facts here are clear cut. A patient came in from another hospital on Wednesday, February 19th—one week before the email—already intubated and on a ventilator, and the doctors at UC Davis—who have treated other coronavirus cases—immediately suspected a coronavirus infection. But the US Center for Disease Control (CDC), the organization with the sole authority and ability to administer a coronavirus test, refused to test.
Why? Because this patient didn’t fit their “criteria” for testing. These criteria—what are known as Patient Under Investigation (PUI) guidelines—have been set in stone in the United States since coronavirus first burst onto the scene a few months back. Do we know for sure that the UC Davis patient was either a) in mainland China within the past 14 days, or b) in close contact with another confirmed case? No? Well then by definition this UC Davis patient could not possibly have a coronavirus infection. No test for you! It’s not that testing was not available. It’s that testing was not allowed.
This policy can be characterised as “Don’t Test, Don’t Tell” and it is the single most incompetent, corrupt public health policy of my lifetime.
But wait, there’s more. It’s not only this patient who was directly harmed by this policy:
When the patient arrived [Wednesday], the patient had already been intubated, was on a ventilator, and given droplet protection orders because of an undiagnosed and suspected viral condition. … On Sunday, the CDC ordered COVID-19 testing of the patient and the patient was put on airborne precautions and strict contact precautions.
Translation: For four days, every healthcare professional treating this patient at UC Davis was exposed to airborne transmission of coronavirus. And so was every healthcare professional at the hospital before UC Davis, particularly during the intubation process. Because the CDC refused to test this patient for coronavirus in a timely manner, all of the doctors and nurses and technicians caring for this patient were put at risk.
Sure enough, over the next few days about 124 UC Davis Medical Center staffers—including at least 36 nurses—were ordered into self-quarantinebecause of their exposure to this one patient. Worse, three staff members at Northbay VacaValley Hospital—the facility where this patient was treated before being transferred to UC Davis—have already tested positive for coronavirus infection, with an unknown number of additional healthcare professionals from that hospital now in self-quarantine. That’s all from one coronavirus infection.
Now imagine this same story repeated day after day across the United States for the past two months, where those infected with the virus fail to receive the care they need, spreading the disease not only to their community when their symptoms do not require hospitalization, but spreading the disease directly to emergency responders and healthcare professionals when their symptoms do. Even today, more than a week after the consequences of Don’t Test, Don’t Tell were revealed in that first case of community-spread coronavirus from Sacramento, the number of tests performed in the US remains extremely low, particularly in states that were caught flat-footed when the CDC abdicated control over test production. Missouri, a state with a population of more than six million, has performed only 17 tests. Michigan, with a population of 10 million, has performed only a few dozen tests. Pennsylvania, with a population of almost 13 million, can perform all of 33 tests per day. Unsurprisingly, these states do not have a confirmed case of coronavirus within their borders.
Now imagine this same story repeated day after day across the globe.
 Diana Lambert
Diana Lambert
As I write this essay on March 5th, there are more confirmed coronavirus infections in Harris County, Texas (five) acquired by Americans who traveled to Egypt than there are confirmed cases within the entire country of Egypt (three). Why? Because Egypt has only tested a few hundred people in this country of 100 million. There are more confirmed coronavirus infections in the city-state of Singapore (three) acquired by Singaporeans who traveled to Indonesia than there are confirmed cases in the entire country of Indonesia (two). Why? Because Indonesia has only tested a few hundred people in this country of 265 million.
With the exception of South Korea and Italy (and perhaps Australia and the UK), pretty much every nation in the world has adopted some form of Don’t Test, Don’t Tell. The offenders include rich countries like the United States and Japan, vast countries like Indonesia and India, communist countries like China and Vietnam, theocracies like Iran and Saudi Arabia, oligarchies like Russia and Nigeria, social democracies like Germany and France. Don’t Test, Don’t Tell knows no geographic or ideological boundary.
And so you might ask: Is this a difficult or expensive test to make? Is there some fundamental reason of technology or economics why a country might find itself forced to pursue a policy of Don’t Test, Don’t Tell? Nope. It’s a relatively simple test to develop and administer in vast quantities. There are probably half a dozen university and industry labs in Jakarta or Nairobi, much less Moscow or Chicago, that could crank out a few thousand test kits per week if they wanted to. Or rather, if they were allowed to.
Now that doesn’t mean that you can’t screw up the coronavirus test if you really set your mind to it. And in fact, that’s exactly what the CDC did in January, when they rejected the World Health Organization’s proposed test panel for SARS-CoV-2 (the official name for this particular novel coronavirus which causes the disease COVID-19) in favor of a gold-plated test panel of the CDC’s own design. After all, why just test for SARS-CoV-2 when you could also test for other SARS and MERS viruses? Unfortunately, with complexity came error, and these initial CDC triple-test kits had a flaw in one of the multiple tests, ruining the entire test. Now the CDC is producing a solo test for the SARS-CoV-2 virus, but this fiasco set us back weeks in test-kit supply.
So if it’s not a difficult or expensive test to make, why are so many countries pursuing a policy of Don’t Test, Don’t Tell? The answer, of course: to maintain a political narrative of calm and competence.
Two weeks ago I wrote about the corrupt political response of China to COVID-19:
A city falls when its healthcare system is overwhelmed. A city falls when its national government fails to prepare and support its doctors and nurses. A city falls when its government is more concerned with maintaining some bullshit narrative of “Yay, Calm and Competent Control!” than in doing what is politically embarrassing but socially necessary.
That’s EXACTLY what happened in Wuhan. More than 30% of doctors and nurses in Wuhan themselves fell victim to COVID-19, so that the healthcare system stopped being a source of healing, but became a source of infection. At which point the Chinese government effectively abandoned the city, shut it off from the rest of the country, placed more than 9 million people under house arrest, and allowed the disease to burn itself out.
And so Wuhan fell.
The disaster that befell the citizens of Wuhan and so many other cities throughout China is not primarily a virus. The disaster is having a political regime that cares more about short-term public and economic concerns than it cares about saving the lives of its citizens.
Aaron Sarin
We must prevent that from happening here—or anywhere. Yes, containment will likely fail. But that does not mean the war is lost. We can absolutely do better—so much better—for our citizens than China did for theirs. China’s handling of the coronavirus in Hubei province, from its muzzling of doctors like Li Wenliang for “rumor-mongering” to its forced quarantines of tens of millions was all guided by Don’t Test, Don’t Tell (with Chinese characteristics).
The Chinese experience with coronavirus is not a “lesson” for the West. It is a cautionary tale. How do we do better by our citizens than China did by theirs? By prioritizing the protection of our emergency responders and our healthcare professionals, through better equipment and facilities, yes, but most of all through better policy and organization, starting with the abandonment of “Don’t Test, Don’t Tell.”
Keep reading
Billy Bunter and the Man from Animal Farm

The Tip of the Iceberg

Three Ancient Ways of War

Crémieux on Fertility Collapse, Ozempic, IQ & Pit Bulls | Quillette Cetera Episode 69
What Is the Point of Anthropology?

Dark Artist
