Narrated
Erasing the Word “Woman”
The desexing of language in women’s health research and care is a story of the marginalisation of science, cultural imperialism, and abuse of power.

{kind=link}
The Origins of Gender Identity and How and Why Language Is Desexed
It has been long understood that the sex of individuals should be made visible in health care documents when sex is relevant, to ensure sex-based needs and rights are not overlooked. Thus, the sexed terms of “women,” meaning adult female people, and “mothers,” meaning female parents, have been central to research, policy, advocacy, and communications regarding female reproduction. However, in recent years, those working in maternal and child health have experienced pressure to avoid these terms and desex our language. This pressure has come about due to the rise in cultural salience, personal application, and institutionalisation of a concept developed in the US called gender identity.
When the term “gender identity” was first used, it described an individual’s knowledge of their sex as male or female. However, the meaning soon changed so that gender identity delineated an internal sense of oneself as living in the social role of a man or a woman. In this way, gender identity became enmeshed with the concept of “gender” developed by feminist philosophers to describe the social expectations of men and women. Current definitions of gender identity tend to be circular and retain reference to sex stereotypes, masculinity, and femininity. Further evolution of the concept has allowed for “non-binary” gender identities and the understanding that gender identity is not fixed but can change over time.
For those who subscribe to gender identity, it is their internal sense of self that makes them a man or a woman rather than biology. Recently, increasing numbers of individuals, particularly in the US but also in other Western nations and beyond, are asserting they have a gender identity in conflict with their sex and so are transgender.
Those identifying as transgender have higher rates of poor mental health and other adverse experiences than the general population and are considered a marginalised and suffering group. Someone who is female but who has a gender identity of “man” may experience great distress if referred to as a woman. Thus, some promote desexed language in a desire to avoid distress and protect those they see as vulnerable.
Other individuals and organisations appear to have a broader intent to marginalise sex and to replace it with gender identity across the board, including in policy and data collection. Of course, to do this, it is necessary to obscure sex in language. Desexing language results in straightforward and clear terms such as “women” and “mothers” being replaced with descriptors referring to physiological processes or body parts or otherwise making sex invisible. These replacements may use technical language or are dehumanising, such as “menstruators,” “birthers,” or “vagina owners,” or inappropriately subsume women into “people” or “parents.” Although both men and women have breast tissue, an association between femaleness and breasts means “breastfeeding” and “breastmilk” may be replaced with words like “chestfeeding” or “human milk.” Finally, the phrases “assigned sex” or “sex assigned at birth” are used to communicate sex is not inherent to individuals but is arbitrarily allocated independent of biology. This decoupling of the word “sex” from sex as a biological variable effectively desexes it.
Table 1 presents some desexed replacement terms used for women, mothers, breastfeeding, and breastmilk. For an ongoing documentation of desexed language in women’s health, see the blog by writer Milli Hill, The Word is Woman (Hill 2024).
Table 1. Sexed terms and their desexed replacements in relation to female reproduction.
|
Sexed terms |
Desexed replacement terms |
|
Women |
People,
individuals, humans, patients, someone, uterus havers, people with uteri,
cervix havers, people with vaginas, bodies with vaginas, birthing bodies,
female-assigned bodies, menstruating personnel, menstruators, bleeders,
menstruating individuals, bodies that bleed, menstruating bodies, people who
experience periods, people who period, people who menstruate, vulva owners,
vulva people, someone with a vulva, birth people, non-males, non-men,
non-prostate owners, individuals who have receptive vaginal sex, womb
carriers, those assigned female at birth, reproductive aged persons
identified as female, person with reproductive potential, person of
childbearing potential, people with reproductive organs, people with
female-identified reproductive organs, individuals who have reproductive
capacity. |
|
Pregnant women |
Pregnant
people, pregnant families, birth givers, gestational carriers, gestational
parents, carriers, gestators, expectant parents, expectant persons, people
expecting, pregnant persons, pregnant patients, childbearing persons,
childbearing individuals, childbearing communities, pregnancy termination
seekers, maternal agent, service users, expectant birthing individuals,
person pregnant, those who labor, people expecting. |
|
Mothers |
Parents,
families, gestational parents, postpartum individuals, postpartum
participant, birthers, birthing parents, postpartum individuals, postpartum
people, caregivers, parentals. |
|
Mother-infant dyad |
Parent-infant pair, postpartum dyad, peripartum unit, lactating dyads. |
|
Breastfeeding mothers |
Breastfeeding
parents, nursing parents, breastfeeding families, breastfeeders, chestfeeding
parents, lactating parents, lactating families, lactators, lactating
individuals, pumping parents, those who are latching their baby. |
|
Breastfeeding |
Human
milk feeding, human milk provision, chestfeeding, lactating, body feeding,
feeding from the body, mammal feeding, feeding, nursing. |
|
Breastmilk |
Human milk, parents’ milk, chest milk. |
Cultural Imperialism and Desexed Language
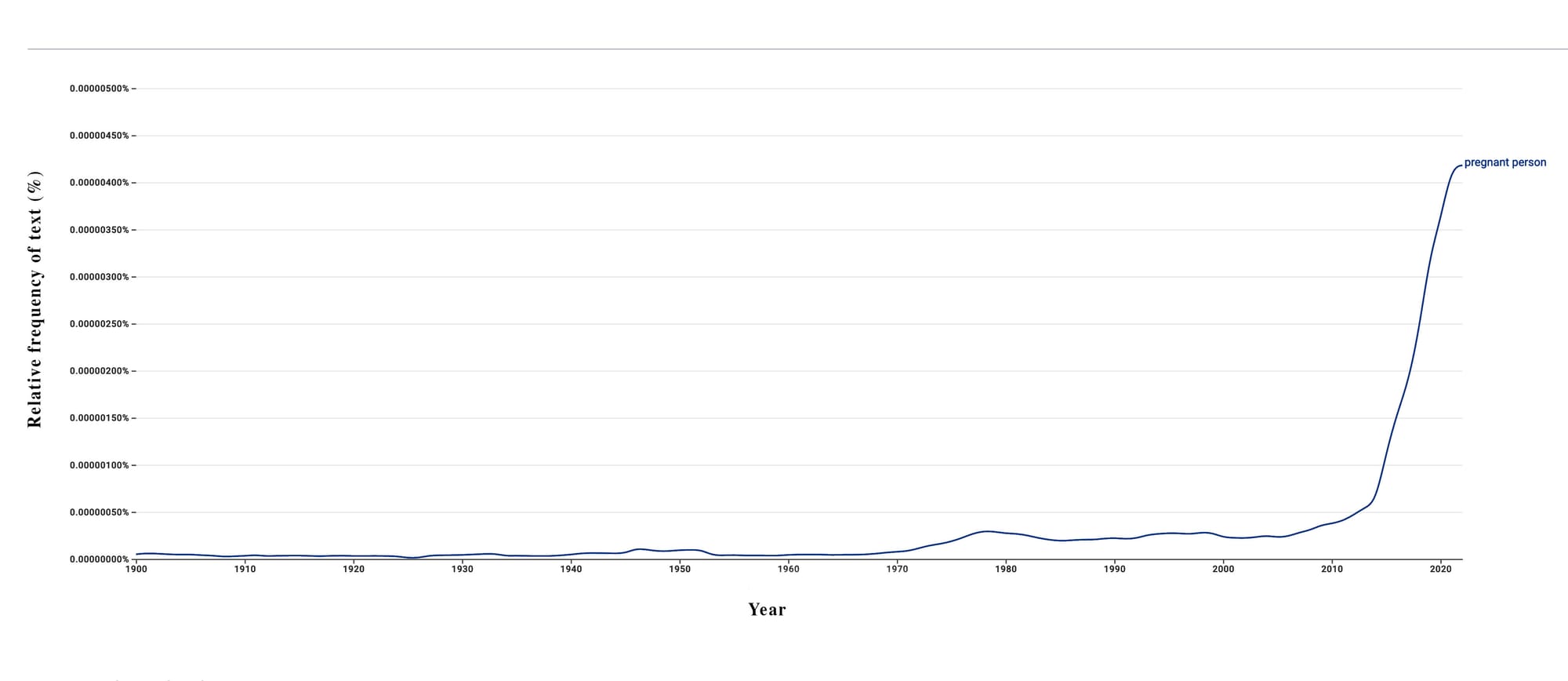
The pressure to desex language has occurred not just in the US but also in other Western and non-Western countries and in and via international organisations through US cultural power. The US origin of desexed language is supported by internet tools showing the uptake and spread of desexed terms. Google Books Ngram Viewer® shows trends in language in the Google Books® corpus. “Chestfeeding” first appeared in Ngram in 2010, and there has been a sharp increase in its use from 2012 until the present. Ngram shows the phrase “assigned sex” as far back as the mid-1800s and “sex assigned at birth” from the mid-1950s in small numbers. The long-term use of these terms relates to infants with disorders or differences of sexual development (DSDs), a small proportion of whom do not have a clear sex, so “assigning” them a sex is accurate. However, since 2010, there has been a sharp increase in the frequency of “assigned sex” and “sex assigned at birth,” reflecting the new use of these phrases to supplant “biological sex” or simply “sex.” Similarly, “pregnant person” has been included sporadically in books since the 1800s, with more consistent use from the mid-twentieth century and a sharp increase in use since 2013.
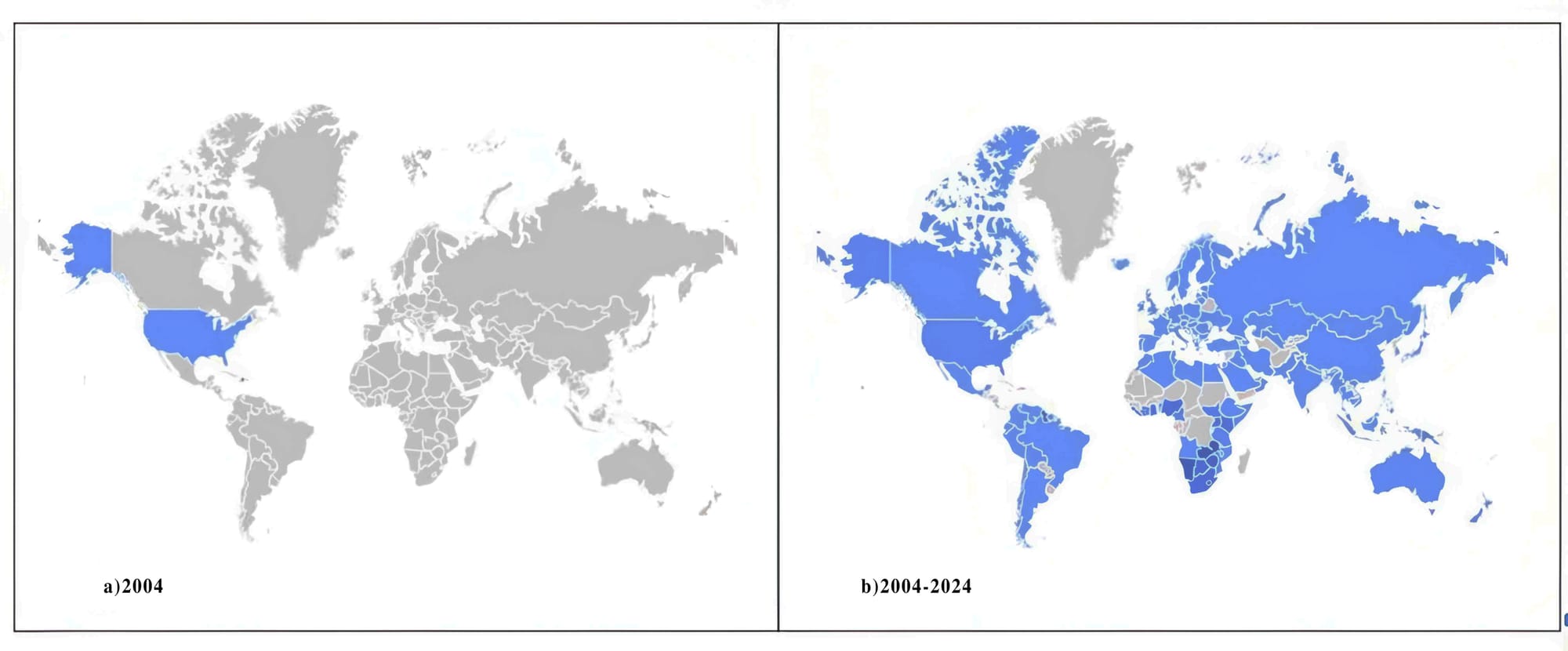
The spread in the use of desexed language can be seen using Google Trends®, which analyses random samples of internet searches to show the popularity of search terms across time and geography. Google Trends® consistently shows the geographic spread over time from the US to across the world of terms like “assigned sex,” “menstruators,” “birthing people,” and “chest feeding” from about 2015–16 onwards.
Growing Pressure to Desex Language
Recommendations to use desexed language started in the US and Canada around 2014–15. This was most visible in relation to the novel term “chestfeeding” and there were a number of papers aimed at health professionals promoting this word at that time. However, research suggests that chestfeeding was not then in widespread use amongst those who identified as transgender. A research team led by Trevor MacDonald considered “experiences with lactation, chestfeeding, and gender identity” of “transmasculine individuals,” but of twenty-two research participants, only three said they preferred the term chestfeeding. Similarly, Michelle Walks wrote a book chapter, “Chestfeeding as a gender fluid practice,” in the Routledge anthology Breastfeeding: New Anthropological Approaches but all study participant quotations referred to breastfeeding and none to chestfeeding. The promotion of chestfeeding by these authors demonstrates how advocating for desexed language may come not just from a desire to support individuals but also to shift how societies conceptualise sex and gender identity and use language in relation to each.
When the idea of desexed language was first presented, it was understood that desexed terms should be used on a one-to-one basis with people who preferred them or in tailored resources for this group. Using preferred terms is an evidence-based tenet of person-centred health care, and tailored resources for groups with particular needs are also common, so this was not objectionable. However, it soon became clear that the desexing of all communications was the end goal. Advocacy for desexing language intensified during the COVID-19 pandemic and has continued since. Below, I describe the process and manifestation of desexing language with examples from journals, publishers, university ethics committees, and health organisations.
Professional Peer-Reviewed Journals and Publishers and Desexed Language
Desexed language became noticeably more common in academic publications during the COVID-19 pandemic and has continued to increase in use since. This can be seen in Google Scholar searches for “pregnant people” for 2018, 2019, 2020, 2021, 2022, and 2023, which yields 340, 439, 852, 1,720, 3,400, and 4,600 publications, respectively (a fourteen fold increase) and similarly for “birthing people” over the same years, which yields 23, 49, 119, 351, 738, and 1,190 publications (a fifty-two-fold increase).
Desexed language can be dehumanising but nonetheless has been published unimpeded by journal review or editorial processes. The Lancet not only published a paper describing women as “bodies with vaginas” but quoted this phrase on the issue cover. Research published in The Lancet Western Pacific described the stigma of menstruation but nonetheless referred to study participants as “menstruators”. In 2021, the Harvard Journal of Law and Gender published a paper by J.C. Nash discussing deficiencies in maternity care for black American women that described them as “birthing bodies.”
Desexing language can introduce errors, and the most important publications in the most prestigious journals have not been exempt. For example, the groundbreaking paper on COVID-19 vaccination during pregnancy by Shimabukuro et al. (2021) in the New England Journal of Medicine miscited research as saying COVID-19 severity was greater in pregnant persons as compared to non-pregnant persons when the comparator was, in fact, non-pregnant women.
Some uses of desexed language in peer-reviewed papers are undoubtedly the authors’ preference. For example, the reasoning for using “obstetric body” to mean women was described in a paper on female reproductive anatomy and clearly came from the authors’ desire to promote gender identity over sex. However, journal reviewers and editors have also played an important role in the increasing use of desexed language. Reviewers not uncommonly ask authors to replace sexed terms like “women” and “mothers” with desexed terms like “birthing people” or “breastfeeding parents.” Sometimes these requests are nonsensical; evolutionary biologist Natalie Dinsdale described how a reviewer for her paper on endometriosis and polycystic ovary syndrome requested “women” be replaced with “people with female-identified reproductive organs.”
Some journals have implemented policies requiring desexed language. I was inside the process of such policy implementation in 2020 as a member of the editorial review board (ERB) of the Journal of Human Lactation (JHL). The JHL ERB was presented with a draft policy on “gendered and inclusive language,” advising authors to prioritise gender identity over sex. The policy stated that authors should not use language implying there are two sexes and that “mother” should be understood and used only to apply to gender identity. Guidance accompanying the policy also stated that “assigned sex” rather than “sex” should be used. I provided feedback to the editor, saying that being able to clearly identify women and mothers in language was important when writing about breastfeeding. I argued some requirements were unscientific and inappropriate for an international journal as they imposed an American/Western philosophy on authors from diverse countries, thus presenting a type of US cultural imperialism. My protests and those of others made no difference, and the policy was implemented. I and two other ERB members who objected to the policy were shortly thereafter removed as members.
Other journals and publishers have instituted similar policies. Recently, The Lancet instructed, “Authors should use the term ‘sex assigned at birth’ rather than ‘biological sex,’ ‘birth sex’ or ‘natal sex.’” It is difficult to comprehend the imposition of the unscientific concept of “sex assignment” and requiring authors publishing in The Lancet to use this term as other than neocolonialism. Nonetheless, the editor of The Lancet, Dr Richard Horton, has written about the importance of decolonisation, stating, “Decolonisation seems an urgent obligation if those who advocate for equity wish to be taken seriously and retain even a vestige of moral conscience.” I cannot see how these conflicting positions can be reconciled.
The publisher Elsevier has produced a template of author instructions for their 2,900 journals using the phrase “sex assigned at birth” and stating sex is not binary. Authors are also required to complete a survey during manuscript submission that presumes gender identity is a universal characteristic and includes no option to indicate the concept does not apply. Thus, Elsevier institutionalises not just desexed language but forces the concept of gender identity on all authors, irrespective of location, culture, or beliefs.
Authors may be asked to desex language by editors at any point of manuscript processing. A paper on pregnancy accepted by the British Medical Journal had all instances of “women” replaced at proofing with “people” by a member of the editorial staff, which was reverted after author objection. An editor at The Lancet Global Health requested that my coauthors and I add “chestfeeding parents” to a letter to the editor on breastfeeding women in the Democratic Republic of the Congo (we declined). Authors from Bangladesh were informed by an editor of a requirement to refer to the “assigned sex” of infants during the last round of review of their paper and felt they must comply. It seems authors from non-Western or non-English speaking backgrounds may have more difficulty understanding and less confidence objecting to such requests.

University Ethics Committees
Some human research ethics committees ask researchers to desex the language used in their studies. The already mentioned Natalie Dinsdale was repeatedly requested by her university ethics committee to desex the language of her study on female reproductive anatomy and function. Over three rounds of revision, the ethics committee questioned the use of “women” and “female” in study materials, while Dr Dinsdale defended her use of sexed language. In the final revision request, the direction was to “remove the references to women,” which was rejected by Dr Dinsdale, who informed the ethics committee their requests were inappropriate, and the study was finally approved. In another case, a researcher was required by her ethics committee to replace “women” with a desexed alternative. The study subsequently had a poor response rate, and complaints were received about language. An ethics variation was sought and granted to reinstate “women,” following which recruitment improved. Relatedly, some ethics committees are discouraging researchers from collecting data on sex, adversely affecting efforts toward closing the female data gap. In some cases, such guidance was developed by diversity and inclusion sections of universities.
Desexed Language within Health Organisations
Desexed language also became more commonly used by organisations over the COVID-19 pandemic. Many used sexed language at the beginning of 2020, but by the end of 2021, desexed language was their norm. The United States Centers for Disease Control and Prevention (USCDC) progressively desexed their COVID-19 breastfeeding guidance from May 2020 to January 2021 with the terms “woman,” “women,” “mother,” and “mothers” replaced with “people,” “person,” “lactating person,” “lactating parent,” and “someone.” At the time (and contrary to the evidence), the USCDC was also encouraging the separation of mothers with COVID-19 from their newborn infants, which impacted practice not just in the US but globally. Alongside this, other health organisations, including the US-headquartered International Lactation Consultant Association, began using ambiguous desexed language, speaking of “breastfeeding/chestfeeding families” and the need to keep “parents and infants together.” Thus, in the midst of a pandemic, when mothers and newborn infants were being separated in unprecedented numbers and advocacy was urgently needed regarding the unique importance of mothers to their infants, the word “mother” was declining in use.
As with scientific publications, organisations introduced errors into communications when they desexed language. For example, the Australian Department of Health desexed its COVID-19 vaccination information for pregnant and breastfeeding women in August 2021. A simple “find and replace” of “women” with “people” made statistics on the increased severity of COVID-19 during pregnancy incorrect. The UK’s National Health Service began progressively desexing public communications on female reproductive health in 2020–21, including the blunder, “8 in 10 people under 40 will get pregnant within 1 year of trying by having regular sex without contraception.”
Many changes made by organisations to public health communications also included technical or dehumanising language. The health information service Healthline referred to women as “vulva owners” on multiple web pages. Health Services Executive Ireland outlined that cervical cancer screening is needed “if you have a cervix” but did not explain that those who have cervixes are women. Sometimes organisations simply avoided giving any indication a procedure might be sex-specific, such as the Canadian Cancer Society, which simply said, “If you’ve ever been sexually active, you should start having regular Pap tests by the time you’re 21.”
In grassroots women’s health organisations, pressure to desex language has caused turmoil. In 2020, the US-headquartered breastfeeding support organisation La Leche League International (LLLI) instituted a policy requiring their communications to include “a variety of terms,” a euphemism for using phrases like “breastfeeding parents” or “breastfeeding/chestfeeding.” In 2021, 250 LLLI breastfeeding counsellors from forty-five countries protested against this requirement, calling it “oppressive and colonialist.” More recently, directors of the LLLI affiliate, La Leche League Great Britain (LLLGB), wrote to the LLLI board saying LLLGB would not use desexed language or provide services to males (LLLI had specified they should assist “everyone” who wants to breastfeed, irrespective of sex.) They pointed out that LLLGB is a UK charity with a registered mission “to help mothers to breastfeed through mother-to-mother support” and is a single-sex organisation. The LLLI board responded by describing the word “mother” as a “roadblock” and suspending the accreditation of these directors. The actions of LLLI in imposing a belief in, and prioritisation of, gender identity across their whole organisation is another clear example of cultural imperialism and abuse of power.
Insight into the process of advancing desexed language within health organisations is provided by Kerryn Drysdale et al., who considered desexing language in health policy, promotion, education, and delivery in cervical cancer screening programmes in Australia. Study participants working in policy, health promotion, health provision, and advocacy spoke in favour of desexing the language of cervical cancer screening. They described negotiation on language continually taking place within their organisations with the point of urgency for change to desexed terminology being reached after a long “slow drip” process. They viewed getting desexed language into guidelines and policy as a way of promoting “top-down” language changes throughout health systems and “pushing the envelope further and faster.” Policy was viewed as a critical axis for change to enable the implementation of desexed language more broadly.
Desexed language in policy is particularly concerning as it might skew health priorities and resourcing, thus “pushing the envelope” from language to practice. One possible vector for change is through women’s health strategies, some of which now use the term “women” to refer to gender identity rather than the female sex. The Women and Girl’s Health Strategy for the state of Queensland, Australia, defines women and girls as “all people who identify as a women or girl.” In this way, males with a gender identity of woman or girl are included. The current strategy does not address male health conditions, but it is not difficult to imagine this may change. In fact, many initiatives previously focusing on women and girls have shifted to include both sexes. The organisation UN Women was established to assist in the implementation of the United Nations Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW). CEDAW is an explicitly sex-based convention; however, UN Women now prioritises gender identity over sex. It describes males with a woman gender identity as amongst the most marginalised women and advocates for their access to resources developed to promote women’s equality, such as female-only spaces and women’s sports.
What Are the Arguments Against Sexed Language?
I have already mentioned a desire to support individuals who identify as transgender is an important motivation for some who advocate against sexed language. Arguments against sexed language are also usually presented within a worldview where gender identity is a universal characteristic of humans through time, culture, and geography and wherein there have always been transgender people. Further underlying beliefs are that gender identity is of great consequence while sex is unimportant and the notion that there are two sexes is a colonial imposition.
These beliefs demonstrate a type of ethnocentrism (using beliefs of one’s own culture as a frame of reference for other cultures) and presentism (application of present-day concepts and values to history) and are not only incorrect but offensive. This is particularly so in relation to the assertion that the fact there are two sexes was unknown outside of Europe until the fifteenth century (i.e., before colonialism) and also that gender identity is universal and transgender people have always existed. In regard to the latter, it is true that across time and cultures, there have always been individuals who don’t conform to social expectations of their sex. However, it cannot be said such people experience a gender identity in conflict with their sex or are transgender. Maori researcher Elizabeth Kerekere pointed out just this, stating that in precolonial New Zealand, diversity of gender expression existed, but there is no evidence of individuals having diverse gender identities. In addition, while there are many cultures providing specific accommodations and status for people (usually androphilic males) who are non-conforming to sex stereotypes, such as the Fa’fa’fine of Samoa or Khawaja Sira of Pakistan, it is a mistake to consider these people transgender. To do so is, as anthropologist Paul Vasey described, “gender colonialism” and also ignores the diminishment of such culture-bound understandings that is occurring as the concept of gender identity spreads.
Nonetheless, these beliefs strongly shape arguments made against sexed language, resulting in predominantly ideologically focused claims rather than evidence-based ones. Examples of ideologically focused claims in a recent publication by Sally Pezaro et al. (as far as I can decipher or represent them) include:
• Making sex invisible in language will reduce sexism.
• Sexed language privileges the power of white men.
• Using sexed language is a politically conservative position.
• Sexed language perpetuates reproductive injustice.
• Recognising in language that it is women who become pregnant and give birth is misogynistic.
Those who argue against sexed language also commonly utilise straw man arguments and may falsely say that those who assert sex is important view the social expectations of the sexes or sexism as immutable when the actual proposition is sex is immutable, not sex stereotypes. Finally, it is often claimed that sexed language was imposed on non-Western cultures via colonialism. This argument is without any basis. Where individuals and organisations from non-Western contexts promote desexed language, a link can usually be drawn to the US/the West. For example, a Nigerian health advocate who referred to women as “menstruators” informed me she used desexed language as she was “privileged…[to] work with Western and ‘woke’ organisations.” In another example, views in favour of desexed language by academics from non-Western backgrounds were put forward to argue sexed language has colonial origins. However, these academics were educated in and living in the US or other Western countries, and the underpinning of queer theory and ideas regarding gender identity in their views is unmistakable. In one case, the academic undertook her graduate studies in gender studies at the University of California, Berkeley, now home of the “godmother of queer theory” Judith Butler.
Importantly, those who argue against sexed language have generally not engaged with the challenges of desexed language flowing from less clear health communications. Sally Pezaro et al. (see above) do not address this issue at all. The Equity and Inclusive Language Toolkit of the US Breastfeeding Public Health Partners advises “mothers” and “breastfeeding” could be replaced with “gestational parent” and “bodyfeeding” but also advises using plain language and avoiding technical terms. There is no discussion on how recommendations for desexed and plain language conflict with one another.
Why Has the Impact of Desexed Language not been Researched?
Perhaps what is most extraordinary about the current situation is the lack of research supporting the implementation of desexed language or documenting the impact of these changes. In our 2022 paper on the importance of sexed language, we proposed that desexed language risks decreasing overall inclusivity, dehumanises women, includes people who should be excluded, introduces inaccuracy, precludes precision, creates confusion, undermines breastfeeding, and works against recognition of the mother-infant relationship. We provided examples where each of these detriments was evident and argued that desexed language would likely have the most impact on the most vulnerable women with low education, health literacy, or language skills or who are marginalised as mothers. We pointed out that desexing language works against well-established public health principles to prioritise plain language in health communications. This paper has now been read or downloaded by more than 200,000 people in over 160 countries, suggesting the concerns we described have resonated with many individuals in many contexts.
However, to date, there are just two studies considering the understandability and acceptability of desexed language; one from the US and the other from Uganda. The US study (sixteen participants) found that confusion resulted if “mother” was replaced with “parent” and that replacing “breastfeeding” with “chestfeeding” or “bodyfeeding” had low acceptability. One woman said she would exit a survey using “chestfeeding,” while another distressingly connected “bodyfeeding” to her experience of rape and said she would reject a survey with this term.
The Uganda study (146 participants) considered the understandability and cultural acceptability of terms including “person with a uterus,” “person who menstruates,” “birthing parent,” and “chest feeding.” This research also found confusion and offence; “birthing parent” was understood to refer to both mothers and fathers and the language itself was described as “disrespectful,” “obscene,” and “shameful.” There is enormous potential for desexed language to contribute to poor individual and population health outcomes if women do not understand communications or are unwilling to engage with health services or research due to the language used.
Given the potential adverse impacts of desexed language, the lack of underpinning evidence leads to two questions: Why are changes being made without an evidence base, and why has research on this subject not been published? Regarding the former, this question was asked by women’s health advocate Ciara Curran to a House of Lords Committee in the UK. Ciara is a bereaved mother who established an organisation called Little Heartbeats to support women experiencing a serious pregnancy complication called preterm prelabour rupture of membranes (PPROM) (“Little Heartbeats”). Ciara told the House of Lords, “I keep being told we need medical research to back any changes and polices, yet no research is in place to support removal of terms like women and mothers from health communications and policy and no one appears to have taken into account impact of the loss of these words on women who have lost babies.” Ciara singled out “bodies with cervixes” as unacceptable and became emotional as she connected desexed terminology to dehumanisation of women during pregnancy and childbirth and her own perception of being seen as “a body on the bed” rather than a woman needing health care when she experienced PPROM. Ciara’s words should be no surprise: researchers have repeatedly heard women who have experienced birth trauma describe feeling dehumanised and treated like “just a body.” Ciara’s distress at desexed language being introduced without research is understandable.
Regarding the question of why research has not been published, first, the controversial nature of this subject has dissuaded researchers. Desexing language has been framed as unequivocally positive and “more inclusive,” while questioning desexed language is bigoted and transphobic. I and other authors of the 2022 paper on sexed language experienced personal insults, attempts to have us deplatformed from speaking events (unsuccessful), and complaints to employers and organisations we work with (also unsuccessful). Two individuals who contributed to this paper withdrew before submission, being concerned about how their university would react, or because they thought being a named author might affect their funding prospects.
Second, research may have been undertaken but not published because negative outcomes to desexed language were identified. Non-publication of negative findings is a well-recognised phenomenon, particularly in pharmaceutical research, but this has also occurred in gender medicine. It was recently revealed that the World Professional Association for Transgender Health had suppressed the publication of papers reporting on commissioned systematic reviews of gender transition treatments because the findings were not as desired.
Third, researchers may have been unable to obtain funding to research desexed language due to ideological capture of funding bodies. I was a co-investigator with very senior and experienced colleagues on two grant applications to the UK’s National Institute for Health and Care Research to consider the impact of desexed health communications on women. Our applications were supported by letters from eleven women’s health organisations outlining the dire need for this research. Both applications were prioritised highly in the initial review stage. However, both were rejected at the funding committee stage. With the first application, reviewers were reportedly “horrified” this research was being proposed; it was “dreadful research”; and the topic itself was offensive. With the second application, reviewers made a series of clearly ideologically based complaints, including that we had used the terms “female” and “woman” interchangeably, had not referred to queer theory, and the research question was not presented in neutral language.
For the record, the research question was: “What are the extent, impacts and implications of de-sexed language in reproductive health communications for women in the UK?” It is hard to imagine a more neutral framing, and indeed, we were approaching this research with genuine curiosity as to what we would find, both positive and negative, about desexed language.
In the absence of research, we are left in a place of unknowing regarding the impact of desexed language. Anecdotal evidence of misunderstanding, aversion, and miscommunication supports adverse consequences. It is likely, for example, that cervical cancer screening promotions describing those eligible for screening as “anyone with a cervix” are not understood by some women. But which and how many women? What are the morbidity and mortality costs resulting from missed screening for women who do not understand these health communications or reject the message? How might misunderstanding or rejection be mitigated? Who benefits from desexed language, and under what circumstances? We do not know the answers to any of these questions. And yet journals, publishers, university ethics committees, health organisations, and others are moving full steam ahead using, promoting, and sometimes enforcing desexed language. This is a completely unacceptable situation. Desexing the language of women’s health is a major intervention, one that should not be made without a strong evidence base.
Taking Action to Uphold Science and Evidence-Based Health Care
In order to protect individual and population health, increased understanding, appropriate policies, and research on sexed and desexed language are required. Those in science and health need to appreciate and communicate the known and potential detriments of desexed language and ensure they are properly considered by decision-makers. Providing concrete examples of problems with desexed language can enable understanding that this is not a simple, risk-free change. In international settings, making clear the difficulties for non-native English speakers and the cultural imperialism of using desexed language can be helpful. I am aware of many meetings where desexed language has been proposed but where individuals have suggested caution, referred to the paper on the importance of sexed language, and sexed language has been retained.
Working together with colleagues can also increase confidence and provide protection. Recently, I collaborated with others in writing and gathering support for responses to two Australian government consultations addressing sexed and desexed language in research and data collection on sex. While the responses were written by a small number, they were endorsed by many (over two hundred). Numerous signatories were cognisant of the challenges of desexed language, but for others, just being asked to consider supporting the responses also performed an educative role.
Journal publishers and editors should implement appropriate policies in relation to sexed and desexed language to guide authors and reviewers. Journals should not permit papers to be published using dehumanising, desexed language. They should have policies preventing authors who have used sexed language in their recruitment and study instruments from using desexed language in their papers as a matter of ethics and respect for research participants. They should not require terms like “assigned sex” or universalise gender identity. They should ensure authors do not feel pressured by reviewers to use desexed language. Where desexed language is used by authors, journals must ensure accuracy is not compromised, nor research of others misrepresented. They should make certain that where “women” has been used in a gender-identity-based meaning (including males), data is nonetheless disaggregated by sex so that sex differences are visible. If disaggregation by sex is not possible because sex data has not been collected, this should be noted as a limitation. The UK Network of Professors of Midwifery and Maternal and Newborn Health has produced a position statement on sexed language which includes recommendations that “journal editors should not seek to influence authors to use de-sexed language” and that “authors of journal articles, policy, health information should avoid language that disembodies and dehumanises people by reducing them to body parts or functions.” A number of women’s health journals are using this position statement to guide their work.
Ethics committees should not outsource guidance development to diversity, equity, and inclusion bodies. Rather, they should develop their own policies prioritising research quality and ethical conduct, including the avoidance of dehumanising language. They should ensure sex data is collected where any of the following may be relevant:
• Physiological/anatomical differences between the sexes
• Social expectations of the sexes or sexism
• Women’s reproductive capacity
• Women’s reproductive work
Ethics committees should also ensure study participants are able to indicate gender identity is not a characteristic applicable to them. (This is also a recommendation of the UK Network of Professors of Midwifery and Maternal and Newborn Health.)
Organisations must ensure they do not impose desexed language upon individuals or other organisations and show cultural respect. Those holding positions of power have a particular responsibility not to act in a culturally imperialistic manner, but this is not occurring. For example, the 2021 HIV Language Guide of the research funder the US National Institute of Allergy and Infectious Disease describes the terms “mothers,” “women,” “girls,” and “breastfeeding” as “stigmatizing terms to avoid.” This guide also states that stigmatising language (including these terms) should not be used in any communications, including grant applications and publications, with no exemption for non-US grant applicants or recipients. This is completely unacceptable. The Ugandan research group cited above noted their motivation to consider the acceptability of desexed language in Uganda being in response to “pressure from journals and some partner organizations” to use desexed terminology. Their research concluded that “the shift towards de-sexed language may be seen as an imposition of foreign values rather than a progressive step toward inclusivity.”
Organisations generally should be extremely cautious about desexing language absent research to evaluate its impact. Applying established health communication principles and using plain and clear language for the majority population and targeted materials for those with particular needs around sex and gender identity is a defensible position.
Those determining research priorities must urgently act to encourage research on the impact of desexed language and ways in which communication regarding sex and gender identity can be optimised. In addition, any ideological capture of funding organisations needs to be undone. The chilling effect of real or perceived ideological capture of universities and funders on the willingness of researchers to undertake controversial research or state unpopular opinions must be recognised, and a culture encouraging dissent cultivated.
We must act with integrity to advocate for a reinstatement of evidence over ideology in science and health care.
This piece first appeared in the anthology The War on Science: Thirty-Nine Renowned Scientists and Scholars Speak Out About Current Threats to Free Speech, Open Inquiry, and the Scientific Process, edited by Lawrence M. Krauss, Post Hill Press (July 2025). It has been lightly adapted for Quillette. Some references have been omitted for ease of reading: you can find the full list of sources here.
Quillette invites thoughtful responses to its essays.
Selected responses are published once per week as part of a curated Letters to the Editor feature. If selected, letters appear under the contributor’s real name and may be edited for clarity and length.
To submit a letter for consideration, please email [email protected].
🎧 Listen to this article — available to paid subscribers.
Keep reading
Capturing the ‘Odyssey’

Biting the Hand

Sex Differences Above the Neck
A Beautiful Odyssey, Made Dreary By Remorse


Men Without Meaning